Srikara Hospitals Madinaguda
+91-7799111005
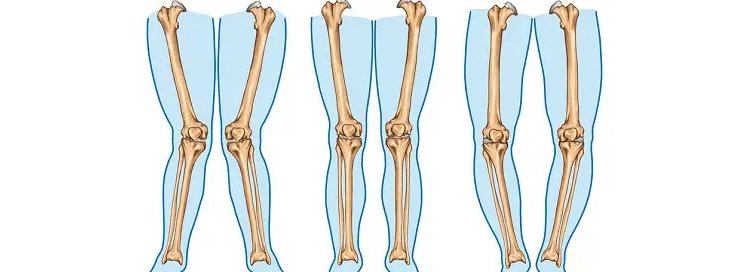
Knee deformities can affect mobility, posture, and overall quality of life. Conditions such as bow legs, knock knees, arthritis-related deformities, and joint misalignment may lead to chronic pain, difficulty walking, stiffness, and reduced knee function. Knee Deformities Treatment Madinaguda focuses on accurate diagnosis and personalized orthopedic care to restore joint stability and improve movement.
Patients with knee alignment problems may experience:
• Knee pain while walking or climbing stairs
• Uneven leg alignment
• Difficulty standing for long periods
• Joint stiffness and swelling
• Reduced flexibility and balance
• Abnormal gait or posture changes
Early diagnosis and treatment can help prevent further joint damage and improve long-term mobility.
Several conditions can contribute to knee deformities, including:
• Osteoarthritis and cartilage wear
• Previous fractures or trauma
• Ligament instability
• Congenital bone alignment issues
• Sports injuries affecting the knee joint
• Age-related degeneration
Treatment depends on the severity of the condition and the patient’s lifestyle needs. Dr. Arun Reddy Vontela provides comprehensive orthopedic evaluation and advanced treatment plans for correcting knee deformities and improving joint function.
• Medication for pain and inflammation
• Physiotherapy and strengthening exercises
• Knee braces and support devices
• Lifestyle and weight management guidance
For severe deformities, surgical correction may be recommended to restore proper knee alignment and reduce pain. Advanced procedures are designed to improve walking ability, joint stability, and long-term knee health.
Patients looking for orthopedic knee specialist in Madinaguda benefit from modern diagnostic methods, personalized treatment plans, and advanced rehabilitation support. The goal is to reduce pain, improve mobility, and help patients return to their daily activities with confidence.
• Improved joint alignment
• Better walking posture
• Reduced knee pain and stiffness
• Enhanced mobility and flexibility
• Prevention of further joint degeneration
Consulting an experienced knee deformity doctor in Madinaguda at the right time can significantly improve treatment outcomes and overall quality of life.
Madinaguda
Srikara Hospitals,
Srikara Hospitals
Mon - Sat: 9:00 Am - 8:00 Pm,
Dr Arun Vontela (Clinic)
Op Timings
6:00 Pm - 9:00 pm.
© All rights reserved by ARUN ORTHO CARE - Designed By Venlax Group.